
By Dr. Kathryn Dundas, MD, CCFP
Sublime Life | The Journal
For decades, cholesterol advice sounded fairly simple.
Lower LDL.
Raise HDL.
Take a statin if needed.
But the science of cardiovascular health — and longevity — has become much more nuanced.
Today we understand that what matters most isn’t just cholesterol levels. It’s the number of damaging particles circulating in the blood, the inflammatory environment inside the arteries, and how our metabolism and mitochondria function over time.
Which is why a new drug currently in late-stage trials — obicetrapib — has caught the attention of many physicians and researchers working in preventive and longevity medicine.
Not because it simply lowers cholesterol.
But because it may influence some of the most important mechanisms we now believe drive heart disease over time.
A New Drug With an Old Idea
Obicetrapib belongs to a class of medications called CETP inhibitors.
These drugs influence how cholesterol moves between lipoproteins in the bloodstream.
Earlier CETP inhibitors failed in clinical trials, so many researchers assumed the entire drug class was finished.
But obicetrapib may be different.
Early trial data suggests it can:
- significantly lower LDL cholesterol
- reduce ApoB, a key driver of atherosclerosis
- lower lipoprotein(a), one of the hardest lipid markers to treat
- dramatically increase HDL
Large outcome trials are still ongoing, so we don’t yet know the full long-term impact on heart attacks and strokes.
But the excitement around this drug highlights something important:
The science of cardiovascular prevention is evolving rapidly.
What Researchers Are Seeing in Early Studies
So why are researchers paying attention to this drug?
In early clinical trials, obicetrapib has shown several promising effects on lipid biology.
When added to standard cholesterol therapy (often statins or statin + ezetimibe), studies have shown approximately:
• 40–50% reductions in LDL cholesterol
• ~30% reductions in ApoB
• ~30–40% reductions in lipoprotein(a)
• dramatic increases in HDL
One reason this drug is drawing attention is that it appears to layer well with existing therapies.
For example, someone already taking:
• a statin
• ezetimibe
• possibly a PCSK9 inhibitor
could potentially see additional LDL lowering with obicetrapib.
Researchers are also watching another marker closely:
Lipoprotein(a), often shortened to Lp(a).
Lp(a) is genetically determined and strongly associated with premature cardiovascular disease, yet historically we’ve had very few tools to lower it.
Early studies suggest obicetrapib may reduce Lp(a) by roughly one-third, which is meaningful.
The Question Researchers Still Need Answered
The most important question in medicine is never simply:
“Does it change biomarkers?”
The real question is:
“Does it prevent heart attacks, strokes, and death?”
To answer that, a large global study called the PREVAIL trial is currently underway.
This study is following thousands of patients to determine whether obicetrapib actually reduces cardiovascular events.
If it does, it could become a significant addition to the preventive cardiology toolkit.
If not, it will join a long list of drugs that improved numbers but didn’t ultimately change outcomes.
This is the reason physicians watch these trials closely.
A Very Interesting Brain Signal
One unexpected observation in early research has been potential effects on Alzheimer’s biomarkers, including reductions in p-tau217, a protein associated with neurodegeneration.
The connection between lipid metabolism and brain health is an active area of research, particularly in people who carry the APOE4 gene variant.
It’s far too early to draw conclusions here — but it’s an intriguing signal that scientists are exploring.
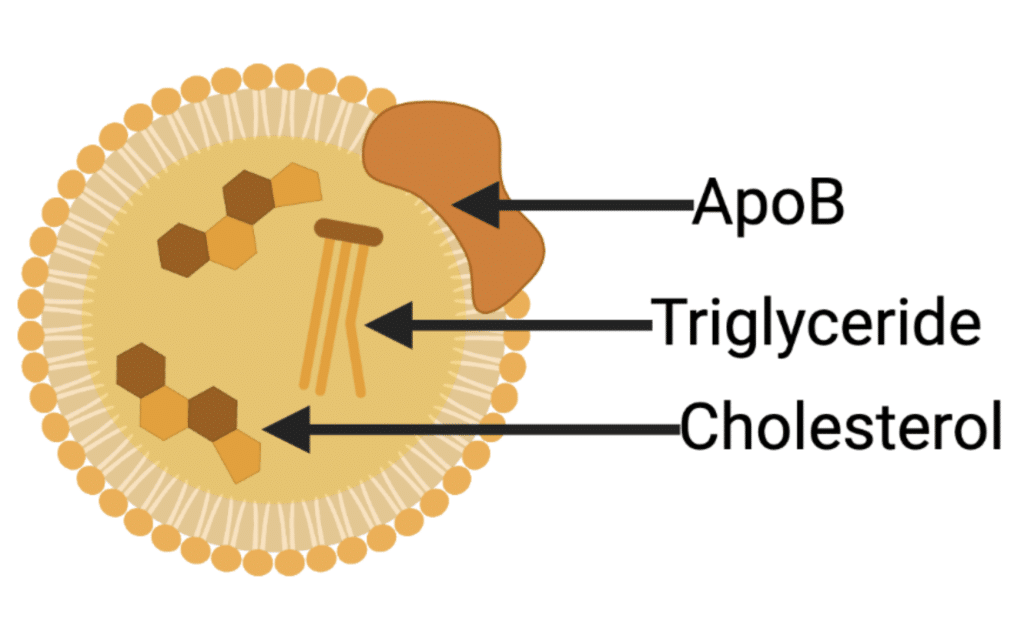
Why Many Preventive Cardiologists Now Focus on ApoB
For decades we focused primarily on LDL cholesterol when assessing cardiovascular risk.
But newer research suggests that what may matter even more is ApoB.
ApoB (apolipoprotein B) is a protein found on the surface of the particles that actually drive plaque formation in arteries.
Each atherogenic particle carries one ApoB molecule, which means ApoB essentially tells us how many plaque-forming particles are circulating in the bloodstream.
Those particles include:
- LDL
- VLDL
- IDL
- lipoprotein(a)
When these particles enter the arterial wall, they can trigger inflammation and the gradual development of atherosclerotic plaque.
So while LDL measures how much cholesterol is inside particles, ApoB measures how many particles are present.
And the number of particles may be the more important risk factor.
This is why many preventive cardiologists — particularly those focused on longevity medicine — increasingly track ApoB as a primary cardiovascular risk marker.
The Real Goal Isn’t Lower Cholesterol
It’s healthier arteries over a lifetime
In longevity medicine we increasingly focus on ApoB and inflammatory burden, not just LDL.
Atherosclerosis begins decades before symptoms appear.
What matters most is the cumulative exposure of your arteries to damaging particles and inflammation over time.
Which is why medication is only one piece of the puzzle.
Many powerful interventions remain surprisingly simple.
The Natural Levers Most People Overlook
Fiber is one of the most powerful cholesterol therapies we have
Soluble fiber helps bind bile acids in the gut and increases cholesterol excretion.
Populations with higher fiber intake consistently show lower cardiovascular risk
Simple targets I often suggest:
- 25–35 grams of fiber daily
- oats, legumes, chia, flax, vegetables
- increasing intake gradually to allow the gut microbiome to adapt
Fiber also improves insulin sensitivity and microbiome diversity, both of which influence systemic inflammation.
Omega-3 fatty acids must reach therapeutic levels
Fish oil is one of the most commonly used supplements — and one of the most misunderstood.
Many people take fish oil but never reach the EPA and DHA levels needed to meaningfully influence inflammation or triglycerides.
Research suggests cardiovascular benefit typically occurs when intake reaches approximately:
2–4 grams of combined EPA + DHA daily.
Quality matters enormously.
Oxidized oils or low-dose supplements simply don’t produce the same biological effects.
At Sublime Life we’ve been working on Vital Omega, designed to deliver clinically meaningful EPA and DHA levels — something many products unfortunately fall short of.
We’ll be sharing more soon, and you can email to join the waitlist if you’re interested.
Food combining can reduce inflammatory spikes
Another concept we discuss frequently in clinic is how foods are combined at meals.
Meals composed mostly of refined carbohydrates can create rapid glucose spikes and inflammatory signaling.
When meals include a balance of:
- protein
- healthy fats
- complex carbohydrates
- fiber
…the metabolic response becomes much more stable.
This translates to lower insulin spikes, less oxidative stress, and less vascular inflammation over time.
CoQ10: the overlooked statin companion
Statins remain one of the most widely prescribed medications in cardiovascular medicine.
But there is an important biochemical effect many patients are never told about.
Statins lower Coenzyme Q10 (CoQ10) levels in the body.
CoQ10 plays a critical role in mitochondrial energy production — the process by which cells generate energy.
Mitochondria are found in the highest concentrations in organs with the greatest energy demand:
• the heart
• the kidneys
• the liver
When CoQ10 levels drop, mitochondrial energy production can become less efficient.
For patients taking statins, I often recommend CoQ10 supplementation to support mitochondrial function and cellular energy production, particularly in the heart.
Practitioner Pick
Three tools I frequently recommend for cardiovascular and mitochondrial health:
- High-quality omega-3 fatty acids providing meaningful EPA and DHA levels – Vital Omega by Sublime Life was developed to provide these therapeutic levels, email to be added to the waitlist.
- CoQ10 to support mitochondrial energy production — particularly for those taking statins
- Fiber-rich whole foods to support lipid metabolism and microbiome health

• Infrared heat therapy such as a Graphene Sauna — gentle deep heat exposure has been shown to support circulation, improve endothelial function, and stimulate cellular repair pathways that benefit both cardiovascular and mitochondrial health.
At Sublime Life we use a Graphene Sauna because graphene heating technology allows for more even infrared penetration and a comfortable therapeutic heat profile, making it easier for many people to tolerate regular sessions. Monthly memberships available.
When these foundations are in place, medications — when needed — often work even more effectively.
A Final Thought
One of the most interesting things about cardiovascular science is how often it reminds us that the body keeps a long memory.
Our arteries don’t just respond to what we do today — they reflect the cumulative story of how we’ve lived for decades.
What we eat.
How we move.
How we regulate stress.
How we support the cellular engines — our mitochondria — that power the heart, kidneys, and liver.
New medications like obicetrapib may become powerful tools, and I’m always excited to see innovation in preventive cardiology.
But the deeper work of longevity often happens in quieter ways — the daily habits that shape the environment inside the body.
When those foundations are strong, everything else we add tends to work better.
And that, ultimately, is the goal:Z
to create the conditions where the body can age well — and where the heart can keep doing its quiet work for many years to come.
Clinical Pearl — Dr. Dundas
When I assess cardiovascular risk in clinic, I’m less interested in a single cholesterol number and more interested in the overall environment inside the body.
ApoB, inflammation, metabolic health, mitochondrial function, and lifestyle patterns all interact over time.
When we address those layers together — nutrition, fiber intake, omega-3 status, movement, and targeted supplementation — we often see lipid markers improve naturally.
Medications can be incredibly helpful tools, but they tend to work best when they’re supporting a healthy system rather than compensating for a stressed one.
Thank you for reading and for continuing to explore the science — and the daily practices — that help us live a Sublime Life.
Warmly,
Dr. Kathryn Dundas, MD, CCFP
Founder, Medical Director, Sublime Life
Make Presence Your Protocol ✦ Sublime Life
Science Corner
Nicholls SJ et al. Obicetrapib for lowering LDL cholesterol. Nature Medicine.
Bhatt DL et al. Omega-3 fatty acids in cardiovascular prevention. New England Journal of Medicine.
Qu H et al. Coenzyme Q10 supplementation in statin therapy. Journal of the American Heart Association.
Pizzorno J. Soluble fiber and lipid metabolism. Integrative Medicine.